Ever heard of the phrase coined by Friedrich Nietzsche, “the devil is in the details”? Professors William Anderson and Boxin Zhao have advanced the battle against microplastic pollution by uncovering the intricate details of how microplastics degrade in the environment. Observation and understanding the fine details of microplastics are key to eradicating them from our environment. The research group has been able to observe the degradation of micro and nanoplastics with unprecedented detail. In collaboration with the National Research Council (NRC) researchers leveraged 3D imaging technology, which allows for a much deeper understanding of the microplastic degradation process than traditional 2D microscopy. This detailed observation is the first of its kind, demonstrating the potential of 3D imaging as a powerful tool in microplastic research.
It’s been quite a while since I’ve posted on this blog, for a variety of personal and some professional reasons. I’ve kept the site alive and functioning (I think?) in the meantime, since the stats show that there continues to be about 100 visitors per day. I guess there is some interest and value in the old posts.
I do intend to start posting again on some sort of regular basis. There are all sorts of topics about engineering (chemical in particular), education, academia, and maybe even admissions, that I have long had plans for. If there are any specific topics of interest to visitors let me know in the comments. See you later!
Once the role of airborne/aerosol transmission of COVID-19 became more recognized, lots of places starting putting HEPA filter devices into offices, classrooms, and various other locations. HEPA (High Efficiency Particulate Air) filters were initially created in the 1940s to help remove radioactive materials from air in labs and manufacturing spaces (during the development of the atomic bomb). Since then they have found common use in labs, manufacturing and other spaces were fine particles need to be controlled, and this includes removal of biological pathogens from air. Generally, a HEPA filter is one that can remove at least 99.97% of 300 nm (or 0.3 micrometre) sized particles from air that travels through it.
At first glance, 99.97% efficiency seems quite impressive and a good level of protection from bacteria and viruses. However, the reality is somewhat more complicated. The basic question is whether your HEPA device sitting in the room is significantly reducing pathogen exposure or not? Like many engineering questions, it depends on the context and here we will explore some of those factors.
A nice article by Prof. Karl Linden at U Colorado, republished from “The Conversation” under CC license. Prof. Linden is a well-known fellow member of the UV research community and IUVA organization. I couldn’t say it any better than him!
Ultraviolet light has a long history as a disinfectant and the SARS-CoV-2 virus, which causes COVID-19, is readily rendered harmless by UV light. The question is how best to harness UV light to fight the spread of the virus and protect human health as people work, study, and shop indoors.
The virus spreads in several ways. The main route of transmission is through person-to-person contact via aerosols and droplets emitted when an infected person breathes, talks, sings or coughs. The virus can also be transmitted when people touch their faces shortly after touching surfaces that have been contaminated by infected individuals. This is of particular concern in health-care settings, retail spaces where people frequently touch counters and merchandise, and in buses, trains and planes.
As an environmental engineer who studies UV light, I’ve observed that UV can be used to reduce the risk of transmission through both routes. UV lights can be components of mobile machines, whether robotic or human-controlled, that disinfect surfaces. They can also be incorporated in heating, ventilating, and air-conditioning systems or otherwise positioned within airflows to disinfect indoor air. However, UV portals that are meant to disinfect people as they enter indoor spaces are likely ineffective and potentially hazardous.
What is ultraviolet light?
Electromagnetic radiation, which includes radio waves, visible light and X-rays, is measured in nanometers, or millionths of a millimeter. UV irradiation consists of wavelengths between 100 and 400 nanometers, which lies just beyond the violet portion of the visible light spectrum and are invisible to the human eye. UV is divided into the UV-A, UV-B and UV-C regions, which are 315-400 nanometers, 280-315 nanometers and 200-280 nanometers, respectively.
The ozone layer in the atmosphere filters out UV wavelengths below 300 nanometers, which blocks UV-C from the sun before it reaches Earth’s surface. I think of UV-A as the suntanning range and UV-B as the sun-burning range. High enough doses of UV-B can cause skin lesions and skin cancer.
UV photons between 200 and 300 nanometers are absorbed fairly efficiently by the nucleic acids that make up DNA and RNA, and photons below 240 nanometers are also well absorbed by proteins. These essential biomolecules are damaged by the absorbed energy, rendering the genetic material inside a virus particle or microorganism unable to replicate or cause an infection, inactivating the pathogen.
It typically takes a very low dose of UV light in this germicidal range to inactivate a pathogen. The UV dose is determined by the intensity of the light source and duration of exposure. For a given required dose, higher intensity sources require shorter exposure times, while lower intensity sources require longer exposure times.
There is an established market for UV disinfection devices. Hospitals have been using robots that emit UV-C light for years to disinfect patient rooms, operating rooms and other areas where bacterial infection can spread. These robots, which include Tru-D and Xenex, enter empty rooms between patients and roam around remotely emitting high-power UV irradiation to disinfect surfaces. UV light is also used to disinfect medical instruments in special UV exposure boxes.
UV is being used or tested for disinfecting buses, trains and planes. After use, UV robots or human-controlled machines designed to fit in vehicles or planes move through and disinfect surfaces that the light can reach. Businesses are also considering the technology for disinfecting warehouses and retail spaces.
The New York City Metropolitan Transit Authority (MTA) is testing the use of ultraviolet light to disinfect out-of-service subway cars. MTA, CC BY-SA
It’s also possible to use UV to disinfect air. Indoor spaces like schools, restaurants and shops that have some air flow can install UV-C lamps overhead and aimed at the ceiling to disinfect the air as it circulates. Similarly, HVAC systems can contain UV light sources to disinfect air as it travels through duct work. Airlines could also use UV technology for disinfecting air in planes, or use UV lights in bathrooms between uses.
Far UV-C – safe for humans?
Imagine if everyone could walk around continuously surrounded by UV-C light. It would kill any aerosolized virus that entered the UV zone around you or that exited your nose or mouth if you were infected and shedding the virus. The light would also disinfect your skin before your hand touched your face. This scenario might be possible technologically some day soon, but the health risks are a significant concern.
As UV wavelength decreases, the ability of the photons to penetrate into the skin decreases. These shorter-wavelength photons get absorbed in the top skin layer, which minimizes DNA damage to the actively dividing skin cells below. At wavelengths below 225 nanometers – the Far UV-C region – UV appears to be safe for skin exposure at doses below the exposure levels defined by the International Committee on non-Ionizing Radiation Protection.
The promise of Far UV-C for safely disinfecting pathogens opens up many possibilities for UV applications. It’s also led to some premature and potentially risky uses.
Some businesses are installing UV portals that irradiate people as they walk through. While this device may not cause much harm or skin damage in the few seconds walking through the portal, the low dose delivered and potential to disinfect clothing would also likely not be effective for stemming any virus transmission.
Most importantly, eye safety and long-term exposure have not been well studied, and these types of devices need to be regulated and validated for effectiveness before being used in public settings. The impact of continuous germicidal irradiation exposure on the overall environmental microbiome also needs to be understood.
As more studies on Far UV-C bear out that exposure to human skin is not dangerous and if studies on eye exposure show no harm, it is possible that validated Far UV-C light systems installed in public places could support attempts at controlling virus transmission for SARS-CoV-2 and other potential airborne viral pathogens, today and into the future.
Emergency hospital during 1918 influenza epidemic, Camp Funston, Kansas. (CC-BY-2.5)
There are some questions about whether the SARS-CoV-2 virus is more or less deadly than the 1918 influenza virus. It’s not really possible to accurately compare the two pandemics’ case and fatality data, for one very big reason. Oxygen!
Today, when someone has any sort of respiratory problem the first likely action is to provide supplementary oxygen. The air we breathe contains about 21% oxygen, which for a healthy person is obviously quite adequate. But for sick people, raising the concentration to near 100% can take the load off their heart and lungs and help prevent other problems like organ failure.
In the 1918 pandemic, the use of supplemental oxygen was not widely known or accepted (as illustrated in the picture, where no one is getting oxygen). There had been some experimentation and use in prior decades (and in treating some chemical weapons victims of the First World War), but it was not yet widespread. Even if it had been enthusiastically embraced, the supplies of oxygen were very limited and it was not readily available on an industrial scale. Therefore we read stories of even young and previously healthy people succumbing to the influenza virus within hours, turning blue due to lack of oxygen in their bloodstream. If oxygen had been available, many of them may have had a reasonable chance to survive and recover. Of course, today we have many other pharmaceutical interventions like steroids and monoclonal antibodies, none of which were available in 1918. But the oxygen is still needed to keep the patient alive long enough so that the pharmaceuticals can have a chance at working.
Where do we get the medical oxygen? There are smaller scale purifying units that take air and concentrate the oxygen in it using membranes to separate the oxygen from nitrogen. These are fine for portable use, smaller scales, or lower flows, but they are not readily scalable to the huge volumes required in a hospital and high-flow oxygen therapy. Likewise, oxygen cylinders are not very practical in hospitals due to their limited capacity. For example, the large “T” size cylinders (about 24 cm diameter by 130 cm tall) only contain about 9,000 L of oxygen once it is depressurized. For patients needing high flow oxygen therapy at up to 60 L per minute, the cylinder would only last about 3 hours or less. If there are a lot of patients, it would take a small army of people constantly moving cylinders in and out of rooms and the hospital. Unfortunately, in poorer and less industrialized parts of the world these options are often the only ones available.
The big industrial oxygen supplies are typically provided in the form of liquid oxygen, shipped and stored in specialized trucks and tanks. The liquid oxygen stored at the hospital is then vapourized into its gaseous form and piped to the patient rooms as required. This is a much more compact and efficient delivery system, since one hundred litres of liquid oxygen expands into about 85,000 L of gaseous oxygen for breathing purposes.
The large scale production and supply of liquid oxygen is a chemical and mechanical engineering accomplishment dating back to the early 1900’s. It took several decades for many plants to be built, with continuous improvements over the years to improve the process and reduce energy requirements. The industrial process uses distillation to separate oxygen from nitrogen (and argon and other trace gases) in air. Since oxygen and nitrogen have quite different boiling points (-183oC for oxygen, and -195.8oC for nitrogen), separation by distillation is a reasonably straightforward approach. However, distillation requires that air be liquified through a combination of pressure and low temperature, and this presents some significant engineering challenges.
Modern plants, often called “Air Separation Units” or ASUs, operate at pressures up to about 6 atmospheres and temperatures in the -170 to -190 range. Clearly it takes some significant compression and refrigeration equipment to carry this out, and the plants are carefully designed to be as energy efficient as possible. The video below, from one major manufacturer, gives a simple overview of the ASU process. Of course, ASUs are built not only for medical oxygen, but also for the many other industrial uses of oxygen such as in steel production, metal cutting, water treatment and chemicals manufacturing.
“In this way you must understand how laughable it is to say, ‘Tell me what to do!’ What advice could I possibly give? No, a far better request is, ‘Train my mind to adapt to any circumstance’….In this way, if circumstances take you off script…you won’t be desperate for a new prompting.”
Epictetus, Discourses
I ran across this quote from the early 2nd century Stoic philosopher Epictetus the other day (“The Daily Stoic” by Ryan Holiday). It reminded me that in engineering education we can’t possibly teach all the information and facts that one might need after graduation. In chemical engineering, for example, there are thousands of different chemicals, types of equipment, different processes for making so many different products. There are different methods for various pharmaceuticals, papers, metals, solvents, plastics, toothpaste, and the list goes on without end. There is a 27 volume Encyclopedia of Chemical Technology that covers many topics in chemical engineering, but even that has its limitations, even if some superhuman could actually learn everything in it. Forty-five years after starting a chemical engineering program in university and I’m still learning new things every week.
So no, we can’t teach everything an engineer might eventually need to know. We probably can’t even teach a small fraction of what people will eventually know or need to use. So we have to focus on training the engineer’s mind. How to approach problems, how to break them down into logical and manageable pieces. How to understand the science behind new situations. How to recognize the limitations of their skills and knowledge, and how they can address those knowledge gaps (it’s important to know what you don’t know!).
So when students of all sorts ask “why do we have to learn this, when are we ever going to use it?”, the answer may well be “possibly never”. But it’s part of the training of the mind, which definitely will get used eventually.
After writing a recent post about helium supply and demand, this news article came up about a new helium production facility in Canada. I wasn’t aware that it was under construction, but it’s nice to see some Canadian progress in securing supplies of this important resource. The photo shows some typical chemical engineering design elements like piperacks, process vessels, separators, compressors, etc. How to put together a process like this, in a safe, sustainable, and economical way, is one aspect of chemical engineering education.
Saskatchewan is now officially home to the largest helium purification facility in Canada after opening in Battle Creek on Tuesday.
Aside from being an English pronoun, He is the symbol for Helium, element #2 on the periodic table. The New York Times article discusses the uses and limitations around He supply, and is an interesting read. Over the last year, I’ve been on a PhD advisory committee for a student in Prof. Steven Young‘s group in the School of Environment, Enterprise and Development (SEED). His student is researching the “industrial ecology” of He, looking into where it comes from, how it’s used, and where the losses occur in the production, transportation and use. It’s quite an interesting issue, and I’ve learned a few things that might be of general interest.
We typically think of Helium use in balloons, or perhaps deep sea diving, but the major worldwide uses are in hospitals (for MRIs), specialized welding and manufacturing, and laboratories (for cryogenics or analytical equipment).
He is collected and purified from natural gas. It is produced during the radioactive decay of uranium in the earth, and collects in pockets of natural gas.
He is one of the few elements on earth that doesn’t have a “cycle”, like the carbon cycle or nitrogen cycle. That means, once it’s released into the air there is no natural way to get it back because it is so light and inert. It simply drifts away into the atmosphere and eventually leaves the planet.
He is so “light” (a small atom) that it is notoriously difficult to contain. It easily leaks and diffuses through materials, even solid metals. That’s why your balloon deflates after a couple of days, and why there are a lot of losses of He during transportation and use.
Since He is so important for some specialized applications, like MRIs, there are concerns that we need to conserve it. Also, since it is associated with natural gas, which we’re trying to scale back because of climate change, it may become more difficult to obtain. It occurs in the air at a concentration of about 5 ppm, so someday we may have to extract it from the air, like we already do with another related element, argon (Ar).
So Helium is kind of an interesting and important material. It involves chemical and mechanical engineering (for extraction, purification, and transportation), physics (for cryogenics, MRI and other applications), and industrial ecology (for understanding how it flows through our global economy, and what might happen in the future).
One interesting topic I come across is “how will our pandemic experience influence technology and design in the coming years“, even after the coronavirus is long gone (preferably) or at least under control? There is a growing awareness that there are things we could be doing better to minimize infection transmission in various commercial and institutional settings, in addition to hospitals where this has been an obvious concern. Even if the coronavirus is completely defeated, reducing the spread of more routine “germs” like colds and influenza or gastrointestinal “bugs” would make good business sense overall, as those account for lost productivity and suffering too. Maybe it’s time we pay more attention to infection prevention in general, beyond just hand washing.
With this interest in mind, I recently agreed to participate on an Advisory Board with a local firm, fabrik architects inc., to provide input on design, materials, and devices that can be used in projects to address the current pandemic and possibly other infection transmission concerns. The Advisory Board members include architects, engineers, and epidemiologists. I look forward to contributing whatever expertise and ideas I have on things like UV disinfection and antimicrobial materials, in what is sometimes called “engineered infection prevention“. It is one way that academics can help to translate current research into new best practices.
Since the pandemic flared in North America, I’ve had quite a few discussions about UV disinfection with media, companies, hospital staff, and various other interested people. There are two major concerns I always try to emphasize:
UV can be an effective disinfection tool IF and ONLY IF it’s used properly (distance, time, power) and at the correct wavelengths (e.g. UV in sunlight, not so good); and
UV disinfection is not safe for the “amateur” user unless it’s been properly designed and engineered into a system that prevents people from exposing their eyes or skin.
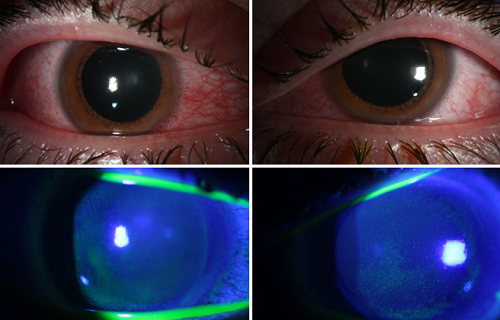
Unfortunately, there are many products now out on the market, widely available to the public, that don’t meet concern #1, or #2, or even both! Concern #1 is not so bad for the public. If someone thinks they are disinfecting something but it actually is doing nothing, then it’s more a waste of time and money than a safety issue (as long as they don’t ignore other infection prevention suggestions). Concern #2 (safety) however, is a more serious issue. And now in the media (as in the link above), we start to see reports of people with eye damage due to these inappropriate (and potentially illegal) devices. This is sad, and has potentially long-term consequences for those individuals.
My recommendation: don’t mess around with UV disinfection unless you really know what you are doing. It’s fine in commercial, hospital, and other installations where it has been properly done. I don’t recommend it for home use in rooms or those hand-held devices. For those who contact me, I’m usually happy to provide quick initial impressions on UV devices and their practicality and safety.








{kind=link}
.png){kind=link}