Once the role of airborne/aerosol transmission of COVID-19 became more recognized, lots of places starting putting HEPA filter devices into offices, classrooms, and various other locations. HEPA (High Efficiency Particulate Air) filters were initially created in the 1940s to help remove radioactive materials from air in labs and manufacturing spaces (during the development of the atomic bomb). Since then they have found common use in labs, manufacturing and other spaces were fine particles need to be controlled, and this includes removal of biological pathogens from air. Generally, a HEPA filter is one that can remove at least 99.97% of 300 nm (or 0.3 micrometre) sized particles from air that travels through it.
At first glance, 99.97% efficiency seems quite impressive and a good level of protection from bacteria and viruses. However, the reality is somewhat more complicated. The basic question is whether your HEPA device sitting in the room is significantly reducing pathogen exposure or not? Like many engineering questions, it depends on the context and here we will explore some of those factors.
A nice article by Prof. Karl Linden at U Colorado, republished from “The Conversation” under CC license. Prof. Linden is a well-known fellow member of the UV research community and IUVA organization. I couldn’t say it any better than him!
Ultraviolet light has a long history as a disinfectant and the SARS-CoV-2 virus, which causes COVID-19, is readily rendered harmless by UV light. The question is how best to harness UV light to fight the spread of the virus and protect human health as people work, study, and shop indoors.
The virus spreads in several ways. The main route of transmission is through person-to-person contact via aerosols and droplets emitted when an infected person breathes, talks, sings or coughs. The virus can also be transmitted when people touch their faces shortly after touching surfaces that have been contaminated by infected individuals. This is of particular concern in health-care settings, retail spaces where people frequently touch counters and merchandise, and in buses, trains and planes.
As an environmental engineer who studies UV light, I’ve observed that UV can be used to reduce the risk of transmission through both routes. UV lights can be components of mobile machines, whether robotic or human-controlled, that disinfect surfaces. They can also be incorporated in heating, ventilating, and air-conditioning systems or otherwise positioned within airflows to disinfect indoor air. However, UV portals that are meant to disinfect people as they enter indoor spaces are likely ineffective and potentially hazardous.
What is ultraviolet light?
Electromagnetic radiation, which includes radio waves, visible light and X-rays, is measured in nanometers, or millionths of a millimeter. UV irradiation consists of wavelengths between 100 and 400 nanometers, which lies just beyond the violet portion of the visible light spectrum and are invisible to the human eye. UV is divided into the UV-A, UV-B and UV-C regions, which are 315-400 nanometers, 280-315 nanometers and 200-280 nanometers, respectively.
The ozone layer in the atmosphere filters out UV wavelengths below 300 nanometers, which blocks UV-C from the sun before it reaches Earth’s surface. I think of UV-A as the suntanning range and UV-B as the sun-burning range. High enough doses of UV-B can cause skin lesions and skin cancer.
UV photons between 200 and 300 nanometers are absorbed fairly efficiently by the nucleic acids that make up DNA and RNA, and photons below 240 nanometers are also well absorbed by proteins. These essential biomolecules are damaged by the absorbed energy, rendering the genetic material inside a virus particle or microorganism unable to replicate or cause an infection, inactivating the pathogen.
It typically takes a very low dose of UV light in this germicidal range to inactivate a pathogen. The UV dose is determined by the intensity of the light source and duration of exposure. For a given required dose, higher intensity sources require shorter exposure times, while lower intensity sources require longer exposure times.
There is an established market for UV disinfection devices. Hospitals have been using robots that emit UV-C light for years to disinfect patient rooms, operating rooms and other areas where bacterial infection can spread. These robots, which include Tru-D and Xenex, enter empty rooms between patients and roam around remotely emitting high-power UV irradiation to disinfect surfaces. UV light is also used to disinfect medical instruments in special UV exposure boxes.
UV is being used or tested for disinfecting buses, trains and planes. After use, UV robots or human-controlled machines designed to fit in vehicles or planes move through and disinfect surfaces that the light can reach. Businesses are also considering the technology for disinfecting warehouses and retail spaces.
The New York City Metropolitan Transit Authority (MTA) is testing the use of ultraviolet light to disinfect out-of-service subway cars. MTA, CC BY-SA
It’s also possible to use UV to disinfect air. Indoor spaces like schools, restaurants and shops that have some air flow can install UV-C lamps overhead and aimed at the ceiling to disinfect the air as it circulates. Similarly, HVAC systems can contain UV light sources to disinfect air as it travels through duct work. Airlines could also use UV technology for disinfecting air in planes, or use UV lights in bathrooms between uses.
Far UV-C – safe for humans?
Imagine if everyone could walk around continuously surrounded by UV-C light. It would kill any aerosolized virus that entered the UV zone around you or that exited your nose or mouth if you were infected and shedding the virus. The light would also disinfect your skin before your hand touched your face. This scenario might be possible technologically some day soon, but the health risks are a significant concern.
As UV wavelength decreases, the ability of the photons to penetrate into the skin decreases. These shorter-wavelength photons get absorbed in the top skin layer, which minimizes DNA damage to the actively dividing skin cells below. At wavelengths below 225 nanometers – the Far UV-C region – UV appears to be safe for skin exposure at doses below the exposure levels defined by the International Committee on non-Ionizing Radiation Protection.
The promise of Far UV-C for safely disinfecting pathogens opens up many possibilities for UV applications. It’s also led to some premature and potentially risky uses.
Some businesses are installing UV portals that irradiate people as they walk through. While this device may not cause much harm or skin damage in the few seconds walking through the portal, the low dose delivered and potential to disinfect clothing would also likely not be effective for stemming any virus transmission.
Most importantly, eye safety and long-term exposure have not been well studied, and these types of devices need to be regulated and validated for effectiveness before being used in public settings. The impact of continuous germicidal irradiation exposure on the overall environmental microbiome also needs to be understood.
As more studies on Far UV-C bear out that exposure to human skin is not dangerous and if studies on eye exposure show no harm, it is possible that validated Far UV-C light systems installed in public places could support attempts at controlling virus transmission for SARS-CoV-2 and other potential airborne viral pathogens, today and into the future.
I’m currently not completely convinced that these “direct air capture” systems that remove carbon dioxide from the atmosphere are very practical. Technically they can certainly work, but the capital and operating costs are probably substantial, compared to the amount of CO2 you recover. However, if they do become widespread (as the linked article suggests), that will keep a lot of chemical engineers busy. And mechanical and electrical engineers too! And civil engineers during the construction phase.
There aren’t very many positive things to say about a pandemic, but perhaps one positive outcome has been the successful advancement of mRNA vaccine technology. Although some people have the impression that this was very rapidly developed over the past year or so, the mRNA idea dates back to the late 1980s. It’s actually been undergoing development for 20+ years, although obviously the target wasn’t always the coronavirus. As a chemical engineer, I’m interested in the scale-up and production aspects, since that’s what we do best.
As a vaccine production method, the mRNA platform is exciting because it is so fast. Traditional vaccine production methods required the growth of batches of cells to produce the vaccine components. This cell growth is done in big tanks, sort of like beer brewing, but is typically slow. It may take many days or weeks to get one batch done. Some vaccines are still produced in chicken eggs (influenza) or cells grown in small “roller bottles” (measles). All of these are slow and difficult to scale-up to produce billions of doses.
The mRNA production method is not cell-growth based, it just uses a biochemical synthesis method. Here, you just mix a bunch of ingredients, add some enzymes to assemble the mRNA molecules, then enclose them in some nanoparticles. These nanoparticles are a key part of the product, and they serve a couple of key roles: 1) they protect the mRNA from degradation, since RNA is fairly unstable especially once injected into your arm; and 2) they provide the mechanism for the mRNA to get into your muscle cells where your body uses it to produce the “antigen” (the piece of virus protein that your body learns to recognize and fight, if you’re ever infected with the virus in the future).
This biochemical synthesis method can be done in a few hours, versus the days or weeks for the traditional vaccine manufacturing methods. There are still some purification and packaging steps involved which take some more time, but the overall process is still very fast in comparison to the older ones. The mRNA platform is very adaptable too, so the vaccine can be quickly modified if necessary, as the virus mutates, just by changing the “manufacturing template” (DNA plasmid) that assembles the mRNA molecules.
The Sartorius company (a science materials & equipment supplier) has produced a short video giving some information about mRNA vaccines and production, which is pretty good and not too technical.
After writing a recent post about helium supply and demand, this news article came up about a new helium production facility in Canada. I wasn’t aware that it was under construction, but it’s nice to see some Canadian progress in securing supplies of this important resource. The photo shows some typical chemical engineering design elements like piperacks, process vessels, separators, compressors, etc. How to put together a process like this, in a safe, sustainable, and economical way, is one aspect of chemical engineering education.
Saskatchewan is now officially home to the largest helium purification facility in Canada after opening in Battle Creek on Tuesday.
Since the pandemic flared in North America, I’ve had quite a few discussions about UV disinfection with media, companies, hospital staff, and various other interested people. There are two major concerns I always try to emphasize:
UV can be an effective disinfection tool IF and ONLY IF it’s used properly (distance, time, power) and at the correct wavelengths (e.g. UV in sunlight, not so good); and
UV disinfection is not safe for the “amateur” user unless it’s been properly designed and engineered into a system that prevents people from exposing their eyes or skin.
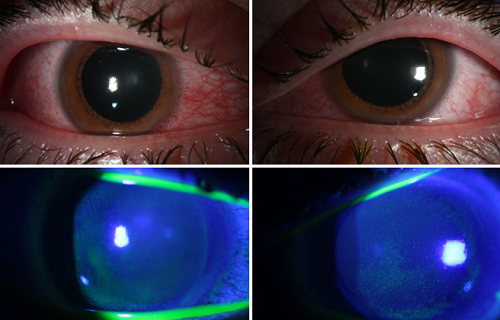
Unfortunately, there are many products now out on the market, widely available to the public, that don’t meet concern #1, or #2, or even both! Concern #1 is not so bad for the public. If someone thinks they are disinfecting something but it actually is doing nothing, then it’s more a waste of time and money than a safety issue (as long as they don’t ignore other infection prevention suggestions). Concern #2 (safety) however, is a more serious issue. And now in the media (as in the link above), we start to see reports of people with eye damage due to these inappropriate (and potentially illegal) devices. This is sad, and has potentially long-term consequences for those individuals.
My recommendation: don’t mess around with UV disinfection unless you really know what you are doing. It’s fine in commercial, hospital, and other installations where it has been properly done. I don’t recommend it for home use in rooms or those hand-held devices. For those who contact me, I’m usually happy to provide quick initial impressions on UV devices and their practicality and safety.
When “chemical engineering” is mentioned, many people think of chemical plants, refineries, and such. That’s one part of it, but it also encompasses many other things, including pharmaceuticals and vaccine manufacture. These days, everyone is talking about and hoping for a vaccine for Covid-19. What does this mean for some chemical engineers and what they need to do?
Recent pandemic developments have strained the supply of N95 filtering facepiece respirators (FFRs), which protect users from particles and aerosols in the air that they breathe. Technically, they must filter out at least 95% of 0.3 micrometre particles.
Normally these are meant to be single-use devices, and are removed and disposed of in a secure way to prevent infection transmission. However, with supply shortages people are considering or resorting to re-using these FFRs, possibly with some sort of chemical or physical disinfection process. Disinfection processes are never 100% effective, so this is not a great option, but I guess it’s better than having no protection.
One disinfection method that I’m very familiar with is UV-C disinfection, having done research in the area of photochemical processes for several decades. There is published literature available demonstrating reasonable disinfection success for UV when applied to N95 FFRs, so this may be an approach to consider if necessary.
I’m working on an overview of this literature (draft version now available at this link), but I’m happy to consult (pro bono) with health care institutions that are considering UV applications to deal with their situations (wanderson@uwaterloo.ca).
With the recent development of a viral pandemic, people are being reminded about the importance of handwashing for infection prevention. Coincidentally, in 2019 my colleague Prof. Marc Aucoin and I supervised a research study on handwashing for the CSA Group, a product standards organization. Specifically, our study aimed to determine if the faucet water flow rate had a significant effect on the ability of handwashing to remove bacteria from the skin.
You can access and read the full report on their website. The bottom line is that no, the water flow rate from the faucet didn’t have a significant effect over the range we tested, from 0.5 to 2.2 gallons per minute (about 2 to 8 litres per minute). Under all of those flow rates, on average about 99.3% of E. coli bacteria would be removed from the hands, which is good to know.
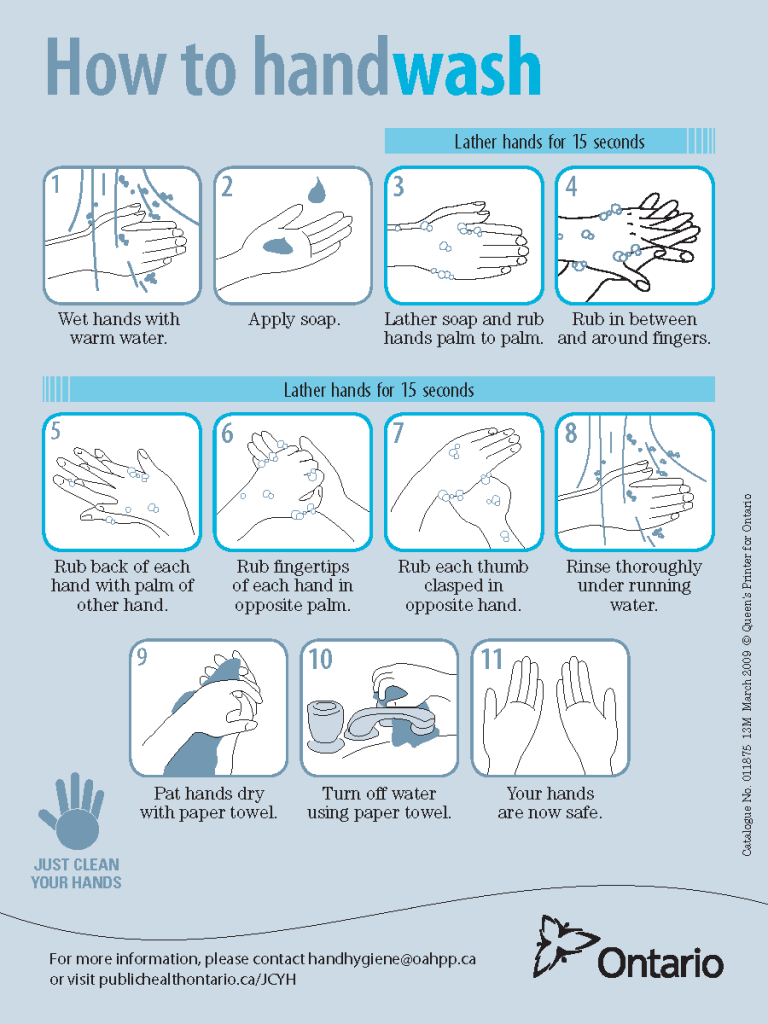
To do this study, we had to control all the other variables as much as possible, including the water temperature, and the amount and type of hand soap used by each person. The other big factor is the way that the hands were washed, including the length of time. For this study, we used a certain protocol from Public Health, and everyone involved in the study learned how to properly wash their hands. This was a good learning opportunity for people, including me, and so I reproduce the protocol that we used below. It’s a useful skill to know how to thoroughly wash your hands these days.
Recommended handwashing technique for infection prevention.
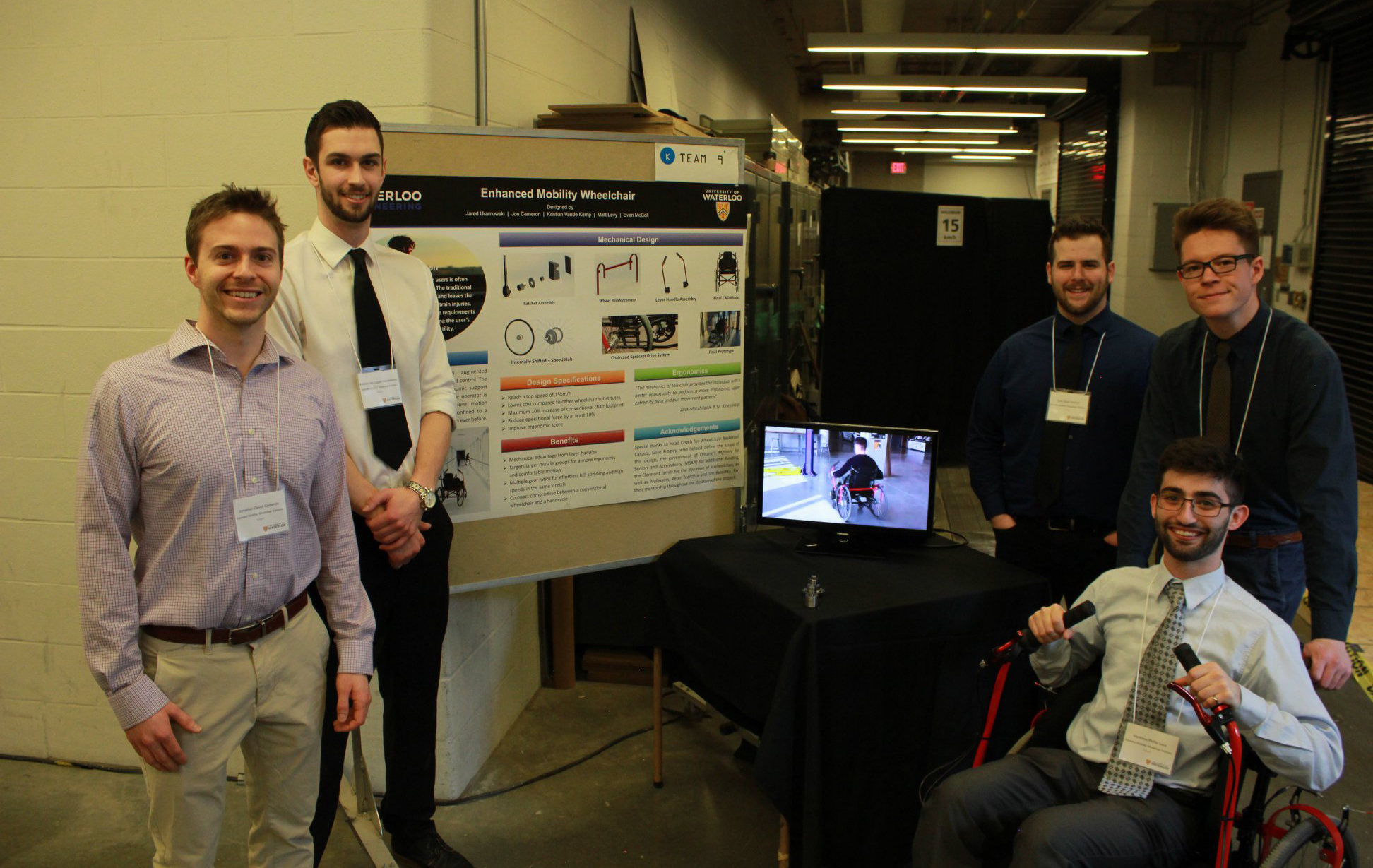
A nice example of mechanical engineering students using their skills to solve real-world problems. See the link below for more details.
Five mechanical engineering students created the Enhanced Mobility Wheelchair for their 2019 capstone design project, and now their work is being nationally recognized for improving accessibility and inclusivity in Canada.
Wheelchair users often face challenges when deciding which device to use to get around. Regular wheelchairs are easy to manoeuvre, but hand-cycle wheelchairs offer better speed efficiency. The Enhanced Mobility Wheelchair team has designed and prototyped an augmented wheelchair that provides users with the comfort and maneuverability of a traditional wheelchair while offering the speed of a hand-cycle wheelchair. The novel drive system provides greater ergonomic support and promotes good posture even when the operator is tired. Selectable gear ratios greatly improve motion efficiency on a variety of terrain, helping those confined to a wheelchair go further and faster than ever before.







{kind=link}
.png){kind=link}